
|
Outlook on life » Should doctors help you die? For and against Death with Dignity Act On October 27, 1997 Oregon became the first state in the United States to legalize the Death with Dignity Act. The law has enabled terminally ill patients with a life expectancy of no more than 6 months to take medications that will end their lives (Ardelt 2003: 429). The fact that only 51% of voters approved the act on a ballot initiative is a strong indication of the polarity between opinions on physician assisted dying in Oregon. It is thus easy to deduce that significant disparities on the topic exist in a more global sense, namely, between individual states across the United States. End of life issues are, in essence, highly complex. Conversations about them can therefore be uncomfortable and difficult, as they pertain to one's deep beliefs and feelings. Notwithstanding these difficulties, though, they are of high value; the course of death-related conversations may eventually lead to discussions on human autonomy or self-determination. Legalization of the Death with Dignity Act remains open to discussion around the United States. Those who contradict the law would claim that the role of doctors is to heal patients, not to help them die which would be the case if they prescribed patients a lethal medication or helped in preparing it. Moreover, they posit that proper palliative care in the final stages of a terminal illness might reduce the need for a hastened death and therefore the government should invest in health-care centres for terminally ill patients. Finally, a corollary of the final stages of life may be life changing experiences enriching a dying person's spiritual life. The Death with Dignity Act, thus, in the opinion of its opponents should not be legalized. Those arguments are, however, based on misconceptions and generalizations that render them spurious. The Death with Dignity Act should in fact be legalized so that terminally ill patients faced with the daunting prospect of imminent death are eligible to make decisions about the time and manner of their death. Doctors would be given the opportunity to fully support their patients by taking into consideration their needs and revering their choices. In no way should such demeanor be viewed as immoral. As a result terminally ill patients would be given the opportunity to live with dignity until the very end if they found palliative care insufficient. The act would also benefit those who feel that their journey in this world has ended, who are in peace with themselves and their loved ones and not expecting any spiritual revelations to come in the final stages of life. Even though physician-assisted dying has been in effect in Oregon for almost 15 years, hastened death is not a novel phenomenon, the history of which should be a starting point in discussion on end of life issues. That history may provide an explanation of fundamental arguments of both advocates and opponents of the Death with Dignity Act and can provide a deeper understanding of the dissent on the issue. 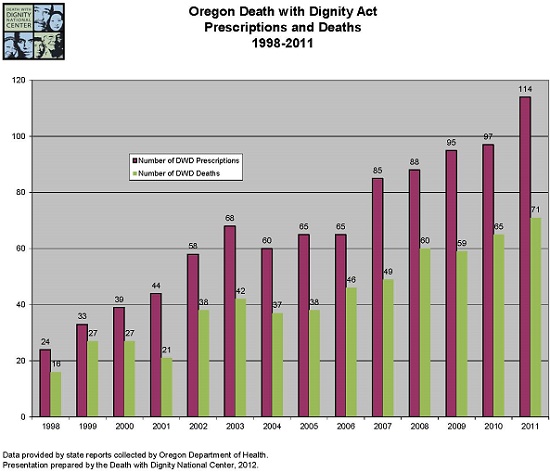 Hastened death was long seen as a positive experience. In ancient Greece and Rome voluntary euthanasia and physician assisted dying were common praxis preserving higher class individuals from extended suffering. Euthansia in Greek means „a good death" (Ardelt 2003: 424). A quote from Gillon on the life of Caesars perfectly epitomizes the attitudes towards hastened death in Antiquity: „As often as Caesar Augustus heard that someone had died quickly and without suffering he prayed for euthanasia for himself." At the time, there were no signs of moral objections against hastened death due to happy and peaceful end it could bring (Rosenfeld 2004: 14). It has to be underscored that such a termination was not only convenient for a dying person but also for the State. Additionally, physicians were eligible to take part in hastening death whereas their help in providing a poison was highly appreciated. More modern practices expounded by Hippocrates ushered a shift in attitudes towards physician assisted suicide. Physicians from a Hippocratic school followed the oath stating that they will never give a deadly drug to a patient, even on a patient's demand. They focused on alleviating pain and maintaining a patient's well-being; physician assisted suicide, hence, was unacceptable for them. Hippocratic philosophy gained credit in the Middle Ages when the sanctity of life was preached and suicide condemned. The Renaissance, however, saw another shift in attitudes towards end of life issues due to developments in education, art and critical thinking as well as gradual liberation from religion. Thomas More in Utopia reiterated ancient philosophers: „If a disease is not only incurable but also distressing and agonizing without any cessation, then the priest and the public officials exhort the man, since he is now inequal to all of life's duties, a burden to himself and a trouble to others, and is living beyond the time of his death, to free himself from this bitter life as from prison and the rack, or else voluntarily to permit others to free him. In this course he will act wisely since by death he will put an end not to enjoyment but to torture." (More [1516] 2005) It was not until the 19th century, though, that a fierce debate over hastened death raged. It was spurred by Dr. Jack Kevorkian who publicly assisted in the death of a terminally ill patient. Another important flashpoint was the introduction of life prolonging medications (Ardelt 2003: 424). As shown above, we are forced to conclude that contemporary arguments for and against the Death with Dignity Act are deeply rooted in the past. To begin with, those against the legalization of the Death with Dignity Act would argue that doctors must always heal patients and help to extend their lives utilizing any means available. The idea of providing patients with medications that will end their lives prematurely is inconsistent with the Hippocratic Oath in that death cannot encourage improvement in a patient's well-being. It is impossible to assess one's condition when that person does not exist (Gill 2005: 62). It has to be underscored, though, that in medicine another basic tenet exists — the principle of beneficience. It refers to any action taken by a doctor to relieve their patient from mental or physical suffering (Rosenfeld 2004: 6). The question arises whether assisting a terminally ill patient in their death may be acknowledged as such a beneficial action. Interestingly, end-of-life interventions do exist in the medical world and are commonly practised. Some of them include: terminal sedation, the withdrawal of life support, and refusal of artificial nutrition and hydration. Proponents the of the Death with Dignity Act would contend that doctors may benefit patients by allowing them to die voluntarily. In the case of terminally ill patients, the only decision they can make is the time and manner of their death. Such patients do not choose death over life as their end is imminent (Angell 2012). We are forced to conclude that the Death with Dignity Act does not necessarily encroach upon a doctor's obligation to benefit a patient. Some of the patients, especially those with a terminal illness, do not find comfort in their relentlessly ending lives and desire to die with peace and dignity. If a patient's decisions took precedence over the medical ethics, doctors would genuinly benefit their patient's well-being. The Death with Dignity Act should thus be legalized so that everyone can enact their inalienable right to choose. Furthermore, opponents of physician assisted dying contend that if proper palliative care was provided to terminally ill patients, the number of requests for earlier death would decrease radically. Such requests are often claimed to be the evidence for inadequate care in hospitals, where patients suffer either physically or psychologically (Rosenfeld 2004: 10). The government, thus, should invest in improvement of places where terminally ill patients spend their last months of life as well as the training of medical staff who care for patients. When the changes were introduced, opponents of the Death with Dignity Act would claim, physical and mental discomforts would disappear along with the need for an earlier death. Notwithstanding a ring of righteous truth to this argument, it neglects to take into account the real nature of physical and psychological suffering in the final stages of a terminal illness. In these final moments, due to the nature of a terminal illness, one thought is found to be prevalent in patients: It is going to be worse every day. Despite the fact that almost all pain may be substantially reduced with modern analgesics, they cannot stop the cumbersome process of dying. „Progressive bodily deterioration can limit and ultimately eliminate one's ability to undertake physical action, and mental deterioration can limit and ultimately eliminate one's ability to make any kind of decision at all. In the end, one may be barely conscious and maintained by machines, bereft of the autonomous nature that gives human beings dignity and inestimable moral worth." (Gill 2005: 56). It is such a tragic end that dying patients desire to avoid. The physical suffering is not a prerequisite though. It is the unconsciousness and lack of control of bodily functions that account for „half-existence". We can see then, that palliative care often fails in the preservation of dignity and the reduction of physical as well as mental suffering in severely ill patients (Angell 2012). Adamant opponents of hastened death may also claim that the end of life period may bring about positive emotional and spiritual revelations. Physician assisted dying might thus bereave dying patients of life changing experiences before death. In the final stages of life such a person might agree with estranged members of family, strengthen or rebuild their relationship with God or another spiritual entity, and establish peace with themselves. In the unique and ultimate situation that death is, such experiences may be particularly intense, and both dying patients as well as their loved ones may benefit (Gill 2005: 59). This way of thinking, however, is faulty in its generalization. Profound and life changing experiences might have already happened for some individuals, they might have already said goodbye to their loved ones or they might not seek a relationship with God at all. Moreover, terminal illnesses are usually long-lasting so the sole experience of pain might have brought spiritual experiences much earlier. What is also worth noting is that in the final stages of life, ill patients might have lost their consciousness. It seems to be impossible for them to experience these profound changes in faltering mental condition (Gill 2005: 59). In some cases then, family may not gain any benefit from observing a painfully dying relative. On the contrary, they may suffer seeing them die in pain. A dying patient, thus, might want to keep their family from painful experiences and remembering their suffering (Steinberg 1988: 142). Throughout the years the Death with Dignity Act has been debated across the United States, especially in the states where it has not been legalized. Adamant opponents of the law would claim that it is morally wrong for doctors to allow patiens to die prematurely. Additionally, good palliative care might reduce the need of terminally ill patients to use the Death with Dignity Act. As a result, patients might experience mental revelations in their life. Although this kind of logic cannot be denied, it fails to take into consideration all patients' needs and beliefs. It may be observed that the Death with Dignity Act may benefit both patients and doctors. Patients and their loved ones, though, are those who the law mostly concerns. It gives them the right to choose the time and manner of their death. It has to be underscored that in such little time as they have left, their choices should be treated with particular reverence. As the law provides terminally ill people with the opportunity to choose their fate in the final stages of life, it should be legalized in every state. References Ardelt, Monika. 2003. „Physician-assisted death", in: Clifton D. Bryant (ed.), Handbook of death and dying. Thousand Oak, California: Sage, 424-434. "Dr. Marcia Angell — May Doctors Help You Die? Physician-assisted Suicide in Massachusetts ". 2012. (You Tube clip, 9 Sep. 2012) (http://www.youtube.com/watch?v=HSDqQCkPabA) (date of access: 11 Nov. 2013). Gill, Michael B. 2005. „A moral defense of Oregon's physician-assisted suicide law", Morality 10, 1: 53-67. Morus, Thomas. [1516] 2005. Utopia. (edited by Henry Morley) The Project Gutenberg. (http://www.gutenberg.org/files/2130/2130-h/2130-h.htm) (date of access: 20 Nov. 2013). Richardson, Peter (dir). 2011. How to die in Oregon. Clearcut Productions. Rosenfeld, Barry. 2004. Assisted suicide and the right to die. Washington: American Psychological Association. Russell, Charlie. 2011. Terry Pratchet: Choosing to Die. KEO films. Steinberg, Donald R. 1988. „Limits to death with dignity", Harvard Journal of Law and Technology 1: 129-162. « (Published: 07-08-2015 )
page 9882 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

| [ Cooperation ] [ Advertise ] [ Map of the site ] [ F.A.Q. ] [ Store ] [ Sign up ] [ Contact ] The Rationalist © Copyright 2000-2018 (English section of Polish Racjonalista.pl) | ||